
Some Facts About Stillbirth
Background
The death of a baby before birth is a tragic event that affects many millions of families each year. There are considerable variation in the definition of stillbirth and in the reporting processes, which makes both determining the size of the problem and international comparisons difficult. The World Health Organisation currently estimates that over 2.65 million babies die every year in the last trimester of pregnancy alone (Cousens 2006). The vast majority of these deaths occur in low to middle income countries (developing countries), accounting for more than 98% of the deaths. Due to under-reporting and unreliable data in many of the countries and regions with the highest incidence of stillbirths, this is thought to be a conservative estimate and the real number may be much higher (Stanton, Lawn, et al. 2006).
In higher income countries, although stillbirths are less frequent, they make up over 60% of all perinatal deaths (deaths in pregnancy and shortly after birth). Stillbirth is now at least ten times more common than sudden infant death syndrome (Smith and Fretts 2007). Over the past two decades, the rate of stillbirth has remained largely unchanged in many countries. Stillbirth therefore also remains a major public health problem in the developed world. A country's stillbirth rates are considered to be the most important indicator of mother and child health.
International comparison of fetal death rate
Table 1. International comparison of fetal death rate at 28 weeks gestation or over, per 1000 live births. A sampling of developed and developing countries. (Sources: McClure, Goldenberg, et al. 2007; Mothers' and Children's Health and Welfare Association Japan 2006)
| Developed Countries | 2004 | Developing Countries | 2004 | |
|---|---|---|---|---|
| Australia | 2.8 | Argentina | 6 | |
| Canada | 3.3 | Bolivia | 11 | |
| Denmark | 4.8 | Brazil | 8 | |
| France | 4.6 | China | 19 | |
| Germany | 3.9 | Egypt | 10 | |
| Hungary | 5.4 | India | 39 | |
| Italy | 3.6 | Ivory Coast | 53 | |
| Japan | 2.2 | Jordan | 13 | |
| Netherlands | 4.9 | Malaysia | 41 | |
| New Zealand | 3.1 | Malawi | 13 | |
| Portugal | 3.4 | Nepal | 23 | |
| Sweden | 3.7 | Pakistan | 22 | |
| U.K. | 3.8 | Papua NG | 28 | |
| U.S.A. | 3.2 | Saudi Arabia | 11 | |
| Zimbabwe | 17 |
Comparison of estimates of stillbirth rates
Table 2. Comparison of estimates of stillbirth rates per 1000 live deliveries at regional levels for the year 2000.
World Region (WHO regions) | Stillbirth rate per 1,000 births | ||
|---|---|---|---|
| WHO estimate | SNL/impact estimate (95% CI) | ||
| World | 24 | 23.9 (18.8-30.5) | |
| HICs | 4 | 5.3 (4.2-6.8) | |
| LMICs | 26 | 25.5 (20.0-32.5) | |
| North Africa | 16 | 18.6 (14.1-24.7) | |
| Sub-Saharan Africa | 34 | 32.2 (25.4-40.9) | |
| Latin America/Caribbean | 10 | 13.2 (10.4-16.7) | |
| East Asia | 19 | 23.2 (18.3-29.5) | |
| South Asia | 34 | 31.9 (25.0-40.7) | |
| Southeast Asia | 18 | 12.7 (10.0-16.0) | |
| West Asia | 16 | 18.9 (14.3-24.9) | |
| Eurasia | 23 | 12.2 (9.5-15.5) | |
| Oceania | 17 | 15.8 (12.4-20.1) | |
Key: SNL/immpact represents a collaboration between Saving Newborn Lives / Save the Children USA and the Initiative for Maternal Mortality Programme Assessment, at the University of Aberdeen, Scotland. HIC: High Income Countries, LMIC: Low and Middle Income Countries. (Reprinted with permission: Lawn, Gravett et al. 2010).
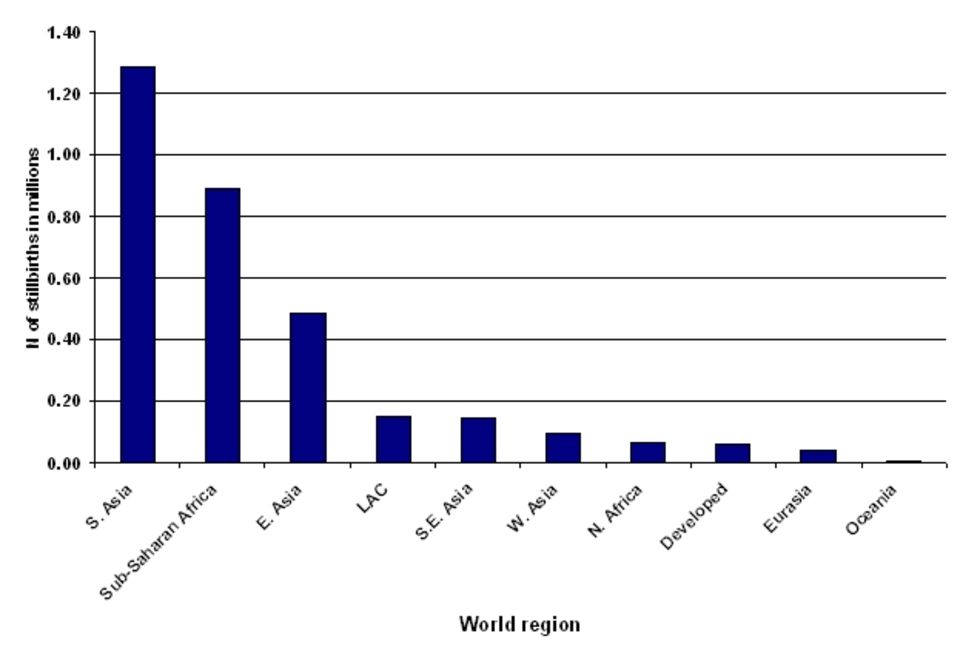
Estimated global number of stillbirths by world region
Figure 1. Estimated global number of stillbirths by world region for the year 2000. (Reprinted with permission: Stanton, Lawn et al. 2006) Click figure to enlarge.
Causes and risk factors for stillbirth
In poorer countries the major causes of stillbirth are: prolonged or obstructed labour, infection, and hypertensive (high blood pressure) disorders such as pre-eclampsia and eclampsia. Approximately 30% of these stillbirths occur during labour and delivery. In wealthier countries fewer stillbirths (about 1.4% in UK; CMACE Perinatal Mortality Report 2008) occur in the intrapartum period, and the major known causes of death are congenital abnormality, spontaneous preterm birth and maternal medical conditions.
Unexplained stillbirth
Depending upon the system used, 20-70% of all stillbirths in the developed world are classified as unexplained. The risk factors that have been associated with unexplained stillbirth include advanced maternal age (over 40; Fretts and Usher 1997; Jacobsson, Ladfors, et al. 2004), obesity (Nohr, Bech, et al. 2005), smoking (Salihu, Shumpert, et al. 2004), fewer than 4 antenatal visits (Huang, Usher et al. 2000), and low socio-economic status (Stephansson, Dickman, et al. 2001). A high proportion of stillbirths which have previously been categorised as unexplained or unexpected are related to intrauterine growth restriction (Froen, Gardosi, et al. 2004; McCowan, George-Haddad, et al. 2007).
Placental pathology is related to risk factors such as smoking, obesity and maternal conditions such as diabetes and pre-eclampsia. The placenta plays a vital role in determining optimal fetal development (Korteweg, Gordijn, et al. 2008) and its role is central to the development of intrauterine growth restriction and other risk factors.
Other less understood risk factors may be abnormalities of the umbilical cord (such as abnormal insertion, hypercoiling of the cord or cord entanglement), resulting in disruption to umbilical blood flow (Hasegawa and Matsuoka 2009). The detection of cord abnormalities through the use of ultrasound is a developing area of interest.
Post mortem
Post mortem and placental pathological examination remain the best investigation for stillbirth. Many stillbirths, however, are not fully investigated and therefore factors relating to the cause of death may well be missed.
Kick counting
Regular fetal movement is acknowledged to be a sign of fetal wellbeing. Pregnancies in which the woman report reduced movements appear to be associated with stillbirth, fetal growth restriction, fetal distress, preterm birth, oligohydramnios and fetal abnormality (Heazell and Froen 2008; Holm Tveit, Saastad, et al. 2009). For this reason there has been considerable interest in reemphasizing the importance of fetal movements as a screening tool for fetal wellbeing.
References
Fretts, R. and R. Usher (1997). "Causes of fetal death in women of advanced maternal age." Obstet Gynecol 89 (1): 40-45.
Froen, J. F., J. O. Gardosi, et al. (2004). "Restricted fetal growth in sudden intrauterine unexplained death." Acta Obstetricia et Gynecologica Scandinavica 83 (9): 801-7.
Hasegawa J, R. Matsuoka, K. Ichizuka, A. Sekizawa, T. Okai (2009). "Ultrasound diagnosis and management of umbilical cord abnormalities." Review. Taiwan J Obstet Gynecol. 48 (1): 23-7.
Heazell, A. E. P. and J. F. Froen (2008). "Methods of fetal movement counting and the detection of fetal compromise." Journal of Obstetrics & Gynaecology 28 (2): 147-54.
Holm Tveit J.V., E. Saastad, B. Stray-Pedersen, P.E. Bordahl, V. Flenady, R. Fretts, J.F. Froen (2009). "Reduction of late stillbirth with the introduction of fetal movement information and guidelines - a clinical quality improvement." BMC Pregnancy Childbirth 9 (32). [Link]
Huang, D. Y., R. H. Usher, et al. (2000). "Determinants of unexplained antepartum fetal deaths." Obstetrics & Gynecology 95 (2): 215-21.
Jacobsson, B., L. Ladfors, et al. (2004). "Advanced Maternal Age and Adverse Perinatal Outcome." Obstet Gynecol 104 (4): 727-733.
Korteweg, F. J., S. J. Gordijn, et al. (2008). "A placental cause of intra-uterine fetal death depends on the perinatal mortality classification system used." Placenta 29 (1): 71-80.
Lawn, Joy E., M.G. Gravett, T.M. Nunes, C.E. Rubens, C. Stanton, and the GAPPS Review Group. (2010) "Global report on preterm birth and stillbirth (1 of 7): definitions, description of the burden and opportunities to improve data." BMC Pregnancy and Childbirth 10 (Suppl 1): S1 [Link]
McClure, E. M., R. L. Goldenberg, et al. (2007). "Maternal mortality, stillbirth and measures of obstetric care in developing and developed countries." Int J Gynaecol Obstet 96 (2): 139-146.
McCowan, L. M. E., M. George-Haddad, et al. (2007). "Fetal growth restriction and other risk factors for stillbirth in a New Zealand setting." Australian & New Zealand Journal of Obstetrics & Gynaecology 47 (6): 450-6.
Mother's and Children's Health and Welfare Association (2006). Maternal and Child Health Statistics of Japan.
Nohr, E. A., B. H. Bech, et al. (2005). "Prepregnancy obesity and fetal death: a study within the Danish National Birth Cohort." Obstetrics & Gynecology 106 (2): 250-9.
Salihu, H., M. Shumpert, et al. (2004). "Stillbirths and infant death associated with maternal smoking among mothers aged >40 years: A population study." American Journal of Perinatology 21 (3): 121-129.
Smith, G. C. S. and R. C. Fretts (2007). "Stillbirth." Lancet 370(9600): 1715-25.
Stanton, C., J. E. Lawn, et al. (2006). "Stillbirth rates: delivering estimates in 190 countries." Lancet 367 (9521): 1487-94.
Stephansson, O., P. W. Dickman, et al. (2001). "The influence of socioeconomic status on stillbirth risk in Sweden." International Journal of Epidemiology 30 (6): 1296-301.
World Health Organization (2006). Journal of Health and Welfare Statistics Vol. 53 (9).
World Health, Organization (2006). "Neonatal and Perinatal Mortality. Country, Regional and Global Estimates." Geneva, Switzerland.